Let’s get this out of the way. Sex is fun. Safe sex is incredibly fun.
The basic rules of sex are “Don’t Do Anything You Are Not Comfortable With”, “Consent is Important” and “Use Protection”. Now obviously there are times when you want to try something new or push your boundaries and that’s fine but remember you are agreeing to a temporary change of your normal rules.
Be clear and be explicit, it’s better than being vague and coy and doing something you were not ready for or not willing to do. If beating women is not your cup of tea then do not agree to flog a consenting partner in a bit of BDSM. And remember, Sex is not A Goal. It is just something two (or more) people chose to do.
These are basics.
When I say “Safety” I don’t mean a hard hat and a harness. Unless that is what your are into. I mean contraception. I mean the prevention of STDs and Babies.
Look babies are nice, but honestly? We insist on a more stringent test for dog ownership than for being a parent. We bombard people with messages about how much hard work it is to have a dog. But we treat children as “toys”. We portray them to the very young as easy and desirable. Yes they are desirable but when you can keep them. Many children learn from pornography and I have nothing wrong to say about porn but porn is an ideal. It’s like the romance where consent flashed through the air through their eyes and their act of sex was precisely tailored to fit both their needs simultaneously. Reality is not like that. Reality is a more trial and error experience, the trick is to make the errors minor and survivable.
If you purchased a husky and have no garden and a tiny flat you would be considered “cruel”. Yet we force young men and women to become parents when they clearly don’t want to or are capable of being parents by reducing the quality of sex education and the quantity of birth control options.
And yes this piece WILL include abortion. But will also include something a lot of Catholics used to flog.
So let’s start with something we fear.
Cumming like a Catholic
These are a set of methods that I term as “catholic” because they were the methods of choice among the more literal minded Catholics who believed that a bunch of celibate men were the best people to give advice on sex.
The two ones note are
Pulling Out
It does what it says on the tin. The two individuals engage in sex and when the time comes to ejaculate, the man simply removes his penis from the vagina. No sperm in the vagina, no pregnancy and no baby. The problem here is that accidents occur. Premature ejaculation is a problem.
When used “PERFECTLY” this method has 4% failure rate. But that’s in ideal circumstances. Typically this has a 22% failure rate.
The Rhythm Method
This is a method based on the cycle of the woman. There are ”safe periods” during a woman’s menstrual cycle during which you can have unprotected sex. This is based on a variety of methods based on cervical secretion, temperature and period of menstrual cycle. The notion is that either there are no available eggs to fertilise or the uterus is not in a state that allows fertilised eggs to implant. This has an ideal failure rate of 0.5 to 1% but in practice it’s 25%.
I do not recommend these methods. They are only effective in an ideal world.
This is where I have to speak about compliance. Compliance is how likely it is for the couple to stick to a specific method of contraception. These methods may have a high theoretical efficacy but in reality they don’t because it’s a system with many points of failure.
For instance? Pulling out does not think about premature ejaculation or indeed getting carried away or the inability to pull out in time. The Rhythm method requires you to be a gynaecologist in order to be perfect at it.
- Can be upto 99% effective
- It takes a lot of time and commitment and education to be effective.
- There are no physical side effects but requires a strict schedule of sex and is less intimate than other methods.
- You have to keep a daily record of your fertility signals, such as your temperature and the fluids coming from your cervix – it takes three to six menstrual (monthly) cycles to learn the method. This I am told is not romantic, but what do those people know.
- Your fertility signals can be affected by factors such as illness, stress and travel or plain perception issues.
- Is absolutely not effective against sexually transmitted infections (STIs).
- Compliance is poor
The major problem with these is that not only are they complicated but they have poor incentives for compliance and are completely ineffective against STD spread.
The Wall
The Barrier Method of Contraception is possibly the most famous because of it’s ease of use and because it actually fights STDs.
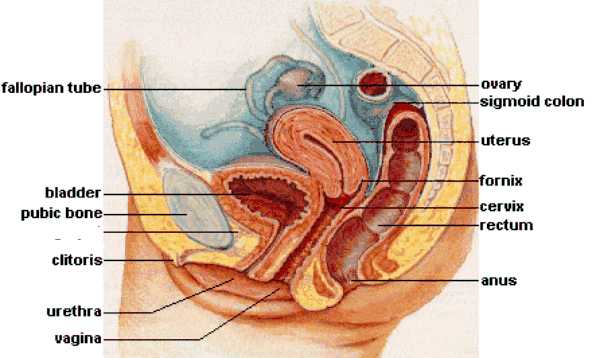
The major list consists of Caps, Condoms and Sponges. And for this we require a little bit of anatomy.
Are we done giggling? Yes? No?
Caps -
These are more of a medical oddity. A historical one especially concerning the rise of reproductive rights.
These were hardened silicone caps that were specially made and fitted over the cervix and held in place by a tense spring against the walls of the vagina. This was then covered in spermicide.
The problem with the caps was that they were uncomfortable. The length of the vagina does vary and can accommodate larger penises but honestly? I can palpate a cervix and even insert a finger into it during childbirth and my fingers are a shade under 4 inches in length. Size isn’t as important as you think but when it came to the cap the penis could easily come in contact with the cap causing discomfort for both parties involved.
But it’s history so we learn about it. This method is as old as civilisation with some practices pre-dating the Bible’s writing. And it was the first contraception BANNED in the USA but it was for a decent reason. The sole manufacturer in the USA was unable to give the FDA a safety profile and efficacy profile. Feminists quickly leapt on it since the Cap was the first method of contraception that was entirely driven by female agency. Unlike the Condom which required male participation, the Cap placed reproductive control in the hands of women entirely. But they weren’t as efficient as we liked, not when the next contender was around. It was legalised in a few short years but it had lost out to the next contender.
Diaphragm -
Similar to the Cap but made out of softer material. This is a specially fitted covering for the cervix. The diaphragm was also preferred by women who had occasional sex and was combined with a spermicidal gel that aided insertion and prevention of pregnancy. It also worked by producing a sperm proof seal to prevent the movement of sperm into the uterus.
This was far more effective than the cap due to high compliance. It was more comfortable and sex was more pleasurable. Women loved it in it’s hey day due to the fact it gave them a good level of protection and they had control over it. However it’s not used all that much due to the invention of the Oral Contraceptive Pill (COCP).
The ideal use is 6% effective and the first year use is around 12% with the problem being poor fitting practice and failure to insert. Some women simply “forget” to put it in. I assume it’s like contact lenses, some days you simply can’t be asked. The diaphragm has a cleaning routine too. It has to be removed daily and cleaned before reinsertion and spermicidal lubricant needs to be applied between intercourse. Like the cap? It must be removed after 8 hours of intercourse. Removing it early can lead to failure.
The problem was this rule didn’t make sense. After all the longer sperm remained surely the greater risk? The thing is it’s the time needed for vaginal secretion and spermicide to destroy the sperm.
Condoms -
The arguable gold standard of the barrier methods. These are basically a sheathe for either the penis or a reversed sheath for the vagina. While the vaginal condom hasn’t captured the hearts and minds of the public, the male condom has.
I suppose the reason for this is that there is a slightly higher failure rate on the female condom and it seems that the application is uncomfortable and the sensation is poor. There are complaints about the male condom but a lot of the male condom’s problem is that people misuse it.
It is a latex or polyurethane or lambskin sheath that is rolled onto the erect penis. After ejaculation it can be rolled off and discarded. Semen doesn’t come into contact with the vagina at all.
Normal use in the first year leads to a 22% chance of pregnancy, however ideal use is just 2%. The problem being erectness of the penis. But what we have to factor in is compliance. Compliance is generally high since the condom is marketed as a method of avoiding the “burden of children” to men. It’s become the premier contraceptive of choice world wide.
With education and proper usage the condom is much much safer than other methods in addition it is highly effective against STDs thus making it the go to method. Now they obviously come in variants but I will say this.
It may not seem like a big deal but oral sex protection is important too. The Condom can form a part of that. While not “ideal” there are flavoured condoms for this purpose.
Sponges -
Another generally abandoned method that consists of a sponge coated in spermicide being inserted to cover the cervix. However due to the lack of proper fit, the failure rate could range upto 24%. This too has generally been abandoned.
Dental Dams -
This is a repurposed medical safety equipment consisting of a latex sheet. A lubricant is applied over the vagina or anus and the dam is placed over it for oral stimulation. This provides the sensation of oral stimulation without the fear of STD transmission. In anal play this is just “safety”.
Gloves -
While we are here we may as well discuss “gloves”. Look, I am not going to tell you that Anal Sex (DUM DUM DUM!) isn’t fun. I have been told that we are undergoing some sort of bumming renaissance and unfortunately the source of this renaissance is 50 Shades of Grey. Now the problem here isn’t that people are rushing out to try anal sex, but they are doing so in a risky fashion. Again they are getting information from what they see on porn too. Well porn actresses and actors achieve a lot of things by the trickery of prep and screen cuts. Not to mention some unsafe practices.
When engaged in anal sex of any sort be it oral, digital or good olde anal sex (mouth, finger, penis) always remember that you need lube and a barrier. Anal sex may be fun but remember it’s not clean and you can catch a UTI or just give yourself bad food poisoning. No one needs that. Be gentle and slow and smart. Dental Dams, Condoms and Gloves are your friends to making what is often a new experience a LOT lot safer. And water or silicone based lubricant is always important.
Now a word about compliance.
The condom is the barrier appliance of choice. But the idea is that the male is responsible for it. A woman cannot possibly be seen being prepared lest either people think she is easy (Oh goodness me! She is getting ready to have sex with strange men!). I think this is nonsense. It’s your bloody vagina, if you don’t guard it yourself then how do you expect some bloke to do it for you? There are no knights in shining armour, if you plan to dance cover his lance.
This is one of the major changes to sex work. Urvasi who helped come up with the concept of this piece advices the young ladies and men who are in the sex work industry and indeed ordinary women who just have sex for fun to make the condom part of sex. Urvasi before she became a woman (the Hijra are Indian Trans People) learnt to apply condoms with her mouth. Now you may say “Avi! What sort of sordid advice is this”, to which I respond “Sensible Ones”. Do not wait for shining knights, take matters into your own damn hands. If you want to have sex and you want it to be safe apply the damn condom yourself. Make sure and it’s awfully hard to argue when it’s part of the foreplay.
If we must teach our young women this then so be it. Better teach them to apply condoms via oral sex than to teach them to care for a child that no one was ready for. Compliance is key and if this increases compliance then why the hell not? Our biggest problem with thinking like this is it is “sexy advice”. People think we are encouraging sex. To which my response is this. Do you think in a piece discussing the amount of agency and responsibility and consent required for sex that I think young girls should be encouraged to have sex as early as possible? Hell No. I think we should teach young kids that sex is normal and natural and that they shouldn’t fear it but should be safe because there are pitfalls to worry about. I would rather they know that things can go wrong and be realistic rather than live in some absurd fantasy where we don’t tell kids how to have sex and then are puzzled that kids manage to do so when it’s something rather ingrained into us as a survival trait.
Safe not Sorry. A Child is for Life.
Now onto our next section.
Eye of Newt, Wing of Bat
No section of contraception is as maligned and misunderstood as the Hormonal or Medical Contraceptives.
These can be effectively divided into
Progesterone Only
The mechanism of action of progestogen-only contraceptives can be divided into
- Very-low-dose progestogen-only contraceptives, such as traditional progestogen-only pills inconsistently inhibit ovulation in ~50% of cycles and rely mainly on their progestogenic effect of thickening the cervical mucus, thereby reducing sperm viability and penetration.
- Intermediate-dose progestogen-only contraceptives, such as the progestogen-only pill Cerazette or the Nexplaxon implant allow some follicular development but much more consistently inhibit ovulation in 97–99% of cycles. The same cervical mucus changes occur as with very-low-dose progestogens.
- High-dose progestogen-only contraceptives, such as the injectable depot preparations, completely inhibit follicular development and ovulation. The same cervical mucus changes occur as with very-low-dose and intermediate-dose drugs.
These have some advantages over the Combined Oral Contraceptive Pill. But requires higher compliance for effectiveness. There is a 3 hour window of effectiveness everyday that the pill must be taken unlike the COCP which has a 12 hour window.
One of the major benefits this has over the COCP is that it isn’t a risk factor for DVT (exercise is important no matter what in it’s prevention) or Hypertension. It also is protective against Ovarian Cancer.
The Combined Oral Contraceptive Pill (The Pill/COCP)
This is one of the most popular forms of contraception. Roughly a 100 million people worldwide use it and it is one of the safest and most effective methods of controlling birth.
Contains progesterone and oestrogen that combine to prevent ovulation and implantation of eggs.
This and the POP above have high effectiveness. First year users have an 8% failure rate. Ideal users have a 0.3% failure rate and compliance is not only easy but high. The pill is based on a 28 day cycle of either 21 or 24 hormone pills and 7/4 placeboes (usually iron pills) which enables the body to mimic the normal cycle.
We cannot discuss the COCP without discussing something about it’s safety. Let’s start with the bad news.
The usage of the COCP does increase the chance of the following
Venous Thromboembolism, Breast Cancer in sensitive women (BRCA 1/2 positive), Hyperkalemia (so not to be mixed with other such drugs like ACE inhibitors), Older Medications used higher doses and could increase depression by dropping seretonin levels, Increased Hypertension and on a more smaller and less worrying scale it leads to increased gallstones and vaginal secretions.
HOWEVER and this is a big whopping however…
The COCP is PROTECTIVE for Ovarian, Colo-Rectal and Endometrial Cancer. In addition it reduces some effects of Polycystic Ovaries and reduces acne. And more importantly we must compare the risks between the two sides. Does the increased risks outweigh the decreased? Yes. It is shown that users of the COCP lived LONGER than the people who did not use it due to these effects.
Now obviously this is because patient selection is important. BRCA1 positive families shouldn’t risk the COCP and should take the POP instead.
The depot preparations, ring, patches and injections work in a similar way.
You Put What? In Where?
The IUD is an interesting little diversion.
The IUD was first designed from a cervical cap that could be inserted and held via the cervix. These work in a simple way.
Any foreign object inserted into the uterus sparks and inflammatory reaction causing the thickening of the uterine wall. The changes to the IUDs have generally been in order to improve that action. The first generation being a simple “foreign body” type implant. The second generation was where these really shone as a long term “fire and forget” type of contraceptive in the Copper T. The copper inhibits sperm motility and this combined could be used for long term contraception and was mainly loved by mothers who wanted to space children.
The current generation involves progesterone impregnanted implants. The progesterone thickens the endometrium preventing implantation and goes by the trade name of Mirena.
It’s good as a system because compliance need not be good. At it’s most basic care consists of proper cleanliness and checking the nylon guide thread. It does require medical installation but it is an outpatient procedure and is done in a few minutes.
The problem I have seen is that some women “forget” all about.
There is an increased chance of Pelvic inflammatory disease, but that’s why hygiene is important.
Along with the birth control implant these have the highest satisfaction and best compliance since it is so easy to follow the routine. And the advantage with the IUD is that fertility is restored within a cycle and pregnancy chance rises to 85% (the normal chance) by then.
Emergency Contraception
This is a combination of the two. The gold standard medical treatment is Mifepristone and the best is the Copper IUD. Mifepristone prevents more than 85% of all pregnancies and the 2nd Generation IUD (or 3rd Gen IUD with Cu) stops 99% of all pregnancies and is added protection for a period of the IUD.
The (un)Kindest Snip
This is the two permanent methods of sterilisation out there.
Vasectomies and Tubal ligations.
They are the physical disruption via surgery of the mechanism of delivery of live sperm and eggs into the reproductive areas. Vasectomies are the preferred method of choice but Tubal Ligations are offered due to their protective effect against ovarian cancer AND because many women prefer to make the decision for themselves.
Long term complications are more in tubal ligation but short term complications are more in vasectomies and it’s mainly swelling, pain and inflammation of the scrotum.
But these are extremely important procedures in controlling one’s potential to bear children. While it doesn’t protect against the spread of STDs, a monogamous couple may opt for this and not utilise any other contraceptives.
Abortion
Abortion is the termination of a foetus either medically, surgically or spontaneously.
Let’s mention this outright. Spontaneous Abortions are the norm. Nearly 50% of all pregnancy are “silent” and end in a spontaneous abortion. If anyone says we are perfectly designed to give birth, they are incorrect. And I will say this. From what we understand in science we classify viability via potential of healthy life. At 24 weeks of gestation this is possible with medical technology. Before that any “baby” is not capable of unique life and is nothing but organising cells. At 24 weeks this distinction becomes life with potential to be human.
In potential isn’t “human”. Otherwise sperm is entirely human. I don’t think we should restrict late term abortion or any abortion for that matter simply because to us it is distateful because most abortions for the purpose of unwanted foetuses are done in the first and second trimester before 24 weeks. No, after 24 weeks an abortion is a tragedy. It is usually either a child that is wanted but the foetus cannot possibly live either due to illness or disability, or a mother dying due to the foetus or the products of shame of rape and incest. Instead we portray it as brutal and soulless and it’s practitioners as monsters rather than reality of late term abortions being a solution to tragedies.
So let’s see….
From the Top!
Medical Abortion
First-trimester medical abortion regimens generally use mifepristone in combination with a prostaglandin analog such as Misoprostol (up to 9 weeks), other options including methotrexate (up to 7 weeks) or a prostaglandin analogue by itself.
Mifepristone/misoprostol combination regimens work faster and are more effective at later gestational ages than methotrexate/misoprostol combination regimens, and combination regimens are more effective than misoprostol alone. Mifepristone/misoprostol can also be used to abort second trimester pregnancies.
The vast majority of abortions are of this kind.
Surgical Abortion
The preferred method of choice and most used is Vacuum Aspiration this is either via manual methods or using an electric pump to remove the foetus, placenta and membranes via the cervix. In some cases this can be used in very early pregnancy.
The second procedure is Dilation and Curettage (D&C) and is a standard gynaecological procedure and is the bread and butter of gynaecology. There in lies the problem. Bans on abortion curtail the usage of D&C for examination of the uterus for malignancy, investigations of abnormal bleeds and so on. Because it can be used to abort. This involves cleaning the walls of the uterus with a curette and scraping the lining off the uterus “off” halting early pregnancies. This is the bare minimum standard surgical abortion.
The bulk of all abortions occur in the first 16 weeks of pregnancy. From then on are late abortions often done due to fears of genetic disorders. From the 15th to the 26th week the method of choice is Dilation and Evacuation. The cervix is dilated and surgical instruments and suction are used in combination to evacuate the contents. Other methods include using prostaglandins to deliver the products of dilatation and evacuation. A form of medical abortion involves the usage of hypertonic amniotic fluid using saline or urea to abort the foetus and then deliver the products via prostaglandin analogue.
Above the 26th week? Well these are the late term abortions. Now the pro-lifers who read this may think that it’s a common thing but sadly it’s not. Out of 1.3 million abortion in the USA just 2000 are late term. The most feared and reviled abortionists do so to save the lives of mothers in medical emergencies. Even “rape and incest” are rarities in this. This is a life saving procedure that saves one life out of two and saves the life that’s most likely to die.
There are three treatments of choice at this time. If the mother can manage to give birth, labour is induced and a live child is delivered. If she cannot? Then there are two choices. Hysterotomy is a C-section under emergency conditions with no care given to the survival of the foetus as the mother is in more immediate risk of death as the foetus itself is dead or dying. However this is a high risk procedure. Still the method of choice are D&E.
But there is one other abortion method that is especially revilled.
It’s code is IDX. Intact Dilation and Extraction. Americans reading this will know it better as PBA or Partial Birth Abortion.
It is a less stressful way to perform an abortion on a mother who is in serious trouble. Remember, late term abortions aren’t because you didn’t use protection but because you wanted a baby and something went wrong and you cannot care for a severely disabled child or your life as a mother (or the life of your spouse or indeed daughter) is now threatened by something like Eclampsia (Pregnancy induced hypertensive seizures) or Placenta Praevia with haemorrhage. These are done to save lives.
Around 0.12% of all abortions are this. But to hear the pro-life side of the argument one would think that every foetus is terminated this way and that obs/gynae encourage this.
The foetus’s skull is not full formed, however the biggest obstacle to delivery is the foetal skull. In some cases the mother is unable to tolerate the delivery of the skull.
You may say “the child can be adopted” or whatever but here is the thing. It is not for us to make such a decision. There is no right decisions here only wrong ones and we may as well take the wrong decision that the mother wishes. And furthermore?
In all the medical literature I have read (And I may be wrong) I have never heard of a single case of a unwanted child being terminated via this method. In every single case it has been a drastic medical emergency in order to reduce immediate maternal mortality and morbidity.
So if the skull doesn’t fit into the girl’s underdeveloped pelvis the foetal skull is decompressed by evacuating the brain via an inserted catheter after an incision via forceps is made. This is obviously horrid imagery of the foetus’s brain being sucked out, but as I said. This is not your choice to make and it’s a tragedy and is treated as one. The imagery of the pro-life’s treatment of such tragedies consists of almost joyous outpourings of faux grief that do nothing but harass those who make this decision. It is with heavy hearts we do this for it is a decision no mother wants to make. The pro-life imagery of this procedure from the standpoint of one who sees the value of it and knows the reasons for it’s usage seems like a gleeful portrayal of witches.
It’s currently used in modified forms in the USA but even that’s dying out. Fairly soon women will not have a quick and easy outpatient procedure to terminate a foetus in a serious complication of pregnancy and have to go through slower methods. Because it’s “inhumane”. But half killing a woman is not?
As I said, there are times when you have no good choices only less bad ones. IDX is just one of those.
So there you have it. A Comprehensive and Short Guide To Safe Sex, Contraception and abortion.
As always, check with your doc to see what’s best for you. Sex is fun, children are fun but a responsibility too. Have them when you can care for them but it doesn’t mean don’t have sex. Abstinence is 100% effective but Sex is a lot more fun and honestly 99.99% effective is pretty good when you are having fun.
Consent, Contraception and Communication are vital to this. You have to tell your kids the truth and the whole truth. You need them to know that sex isn’t scary or “magical” but natural and fun but should be respected. You need to guide them. You can leave it up to teachers but you are responsible for your kids. And part of that is not terrifying them out of something you enjoy but teaching them to respect themselves and to enjoy it when the time comes and not bow to peer pressure and to be safe.
You cannot wrap them in cotton wool and expect them to be forever safe. They will make mistakes and it is better their mistakes have no long term repercussions.
A baby as a punishment is just idiotic. Not only is the underaged parent’s lives affected but so is the baby’s.
But how do you do this? Be engaging. Laugh about sex. Sex is HILARIOUS! If you cannot laugh about sex then what can you laugh about? Yes. It is awkward. Yes. You feel and probably look like an idiot. But if even a little bit of that sinks into their thick teenage heads through all their Twilights and their Macklemores then our job is bloody sorted!
So if you like this? Pass it on. Laugh at it and think like a corkscrew.
It’s your bodies you should be responsible for it. Men? Carry a condom. Women? Carry a condom, use the pill. Combine the two for the safest protection out there. If you aren’t planning to have kids for a while? Get an IUD. Be pro-active. It’s your life and it’s your future.
You may not want children today but one day you will and on that day you will be the BEST parents you can be because right now you know that you aren’t the best you can be. And you know that one day you will be better.
And you know what? That doesn’t make you a whore or a slut or a slag. You know what I call a young boy or girl who not only takes care about their contraception as well as STD protection irrespective of sexuality or orientations? One who thinks that they will have kids when they are good and ready and have found the right person and think about financial security? Do you know what heinous and terrible word I use for such people?
Responsible